 Freelance
Traveller
Freelance
TravellerMedevac!
This article originally appeared in issue 012 of Cepheus Journal, and reprinted with permission in the July/August 2023 issue. The material beginning with the section NPCs was submitted separately by the author after reprint permission was obtained.
This adventure is for 16 players on a world at tech level 314 and a population of 6+. A balkanized world (Government Code 7) would work well but any world where rebels or insurgents against the worlds government are possible would also be an option. Cepheus Engine rules have been used (specifically Cepheus Deluxe) but this should be easy to convert to classic 2D6 roleplaying games. A slightly shorter version was originally published as an Amber Zone competition entry.
The Referee should determine how offworlders are marked as different to locals. Options include: clothing (Easy), mannerisms (Average), accent (Average), facial features (Difficult), bodymorphology (Formidable) or any combination of those (Impossible) pick or use 1D. Use the task difficulties for a Deception throw (unskilled: DM 0 instead of 3) to disguise a PC at ranges down to 5m; use one difficulty level higher for encounters closer than 5m.
Note the Law Level of the world and how the PCs are armed, if at all, outside starport environs.
Players Information
One of the PCs has injured their little finger in cargo loading. One of those freak accidents where no one is to blame, it just got caught awkwardly. (Alternatively, the accident occurred during R&R in an aquapool on a slide, or during sports activity, or combat). At first, it simply appears to be a sprain but within 24 hours has swollen nastily and is heavily bruised. Fortunately, it is the little finger, on the nondominant hand and the PC isnt a concert pianist.
For best effect, treatment is required within a week to ten days although depending on the worlds model of medical care this may or may not be easy to achieve particularly if other, more serious trauma cases are arriving thick and fast.
Referees Information
Select a PC randomly, or have players make a DEX throw and take the lowest score as the victim. Medicine 3 will be able to tell from the lack of pain in the palm and other indications that its most likely broken, and treatment is required, Medicine 2 will be suspicious of this, Medicine 1 will be unsure without further tests. In fact, xrays or scanning tech will reveal it is not only broken but requires surgery to mend. Assuming the PCs dont have access to a fully equipped surgery and a Medicine 3, DEX 8+ surgeon, then a visit to the local Accident & Emergency unit/hospital will be necessary. If one of the PCs is such a surgeon, then consider randomly selecting that PC as having the injury. Also, consider their specialism. A hip specialist on duty in the Fracture Clinic may not think surgery is required at all; a hand specialist may disagree.
AT TL35 theres a 50% chance treatment will result in such damage that amputation is necessary, or that the only treatment is strapping it to the next finger and hoping it heals with some degree of future use (DEX1). Note that anaesthetics only appear at TL4 and can be assumed to be primitive, risky and possibly ineffective even at TL5. At TL610 treatment involves a day surgery operation under general anaesthetic to repair the break with two small (2mm) pins and some soft tissue repair with a 97% chance of near full recovery (roll 2 on 2D for DEX1). At TL11+ tissue and bone reconstruction are an hour long outpatient appointment under local anaesthetic and full recovery.
Diagnosis is by a preliminary examination, xray and basic strapping with referral to a Fracture Clinic and specialist review within 1D days. The Referee may extend this by another 1D days if desired as the Fracture Clinic declines to recommend the patient for local surgery due to being an offworlder and needing to use a starport facility where essentially they will start over. The Fracture Clinic will arrange a Day Surgery date and time (TL610) or a hospital stay of 1D+1 days (TL35). Surgery and Day Surgery will involve a complete fast from food after 7am and liquids after 10am. Day Surgery will be scheduled for a morning session or an afternoon session and will involve a 1D hour(s) wait in surgical gown most likely with other patients describing what their procedures are going to be in all too graphic detail. Referees can make as much or as little as they wish of the world having
- free health care at point of need;
- free health care at point of need but only for certain individuals (e.g. planetary inhabitants);
- pay per use health care;
- or some form of subsidized cost.
Payment, if required, may not be in cash but could be in services rendered, barter, or community service.
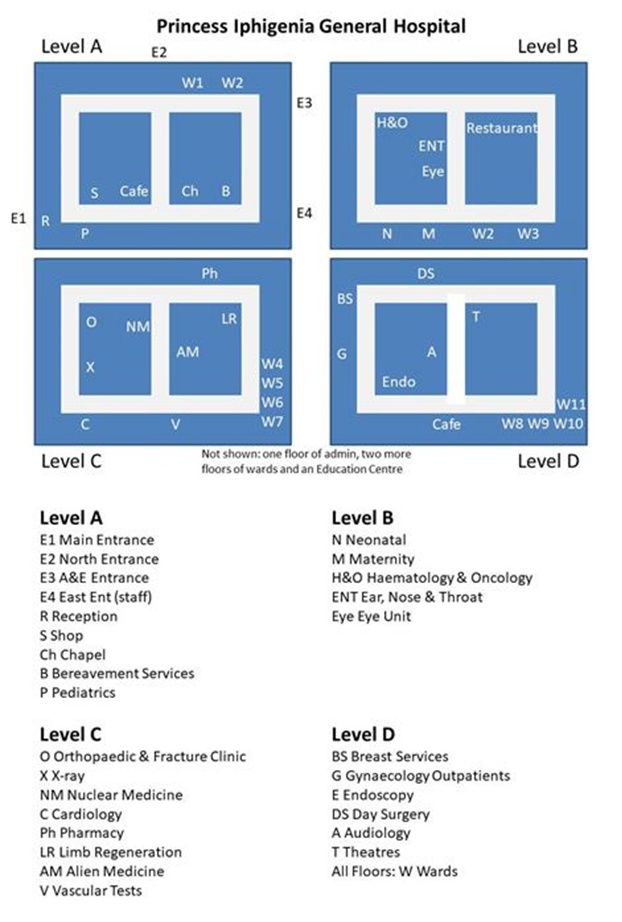 The Princess Iphigenia Hospital
The Princess Iphigenia Hospital
The Princess Iphigenia Hospital, known locally as Pee Eye, is a general hospital serving around half a million sophonts, with some 7000 staff, 600 volunteers, 1200 beds and 28 theatres.
The hospital is shown in an approximate plan of four of its levels which should not be considered exhaustive. Despite the simplicity of the main corridor architecture, the indicated units, wards, surgical areas and so on may be quite labyrinthine entities by themselves with their own receptions, waiting rooms, consultation rooms, curtained cubicles, offices, nursing stations, storage rooms, cleaning facilities, alcoves, etc. At TL35 there will only be stairs, at TL69 there will be stairs and lifts, at TL1014 there will be gravlifts and possibly stairs. Assume lifts/stairs in each corner and near the end of each cross-corridor (i.e. six in total). Additionally, some may be staff only and sized for stretchers or gurneys but may not traverse all floors.
At low Law Levels with limited Government control there may be a small cadre of volunteer protection officers with access to tech level appropriate weapons.
At TL35 PI is a monolithic building built in the grand style
At TL610 PI is a ferrocrete brutalist structure that once won a design award but is now hopelessly out of fashion and aging badly
At TL1114 PI is a sleek, glass-fronted building (and at TL14 may be a gravity hospital, constantly in motion, serving the populace where the need is greatest). At these tech levels assume Level A is the top floor of the building served by gravitic patient/visitor and emergency vehicles landing on the roof.
At tech levels beyond this, hospitals may become a thing of the past with personal and immediate care a basic sophont right.
Referees might wish to add other units as they see fit: Rheumatology, Diabetes & Endocrinology, Orthotics & Blood Tests, Dietetics & Nutrition, Neurophysiology & Urology, and Renal are just some possibilities. Higher tech level options might include cancer day treatment, nerve refusion units, cloning and genetic engineering. Lower tech levels may preclude some units or only have them with very basic facilities (e.g., Limb Regeneration as simply prosthetics).
The PCs may be able to speed or smooth the way by offering assistance with their own skills: Admin, Leadership, Medicine or perhaps even Deception or Liaison. Science type skills in the life sciences should probably count as negative DMs on interactions as medical staff feel their professionalism is being questioned or impugned. Fighting their way through The System will be hampered by two complications. One minor, one major.Its Complicated
The first is that on this world, medical staff are divided into Guilds (TL35), Divisions (TL610) or Cohorts (TL1114). Surgeons, anaesthetists, nursing staff, radiologists, service staff are all very clearly demarcated by any or all of dress, badges, language (i.e., jargon), even when socialising outside the hospital. Unfortunately, at PI relationships have broken down between these groups and theyre barely functioning, never mind being a smoothrunning entity. Pay structures are complicated and surgeons begrudge cleaners being paid more in certain circumstances, trade union talks have broken down and news media is getting wind of the near total breakdown of staff relations and are beginning to ask questions. Recovery rates for patients are at rock bottom. A Difficult SOC roll may allow the PC to avoid much of the game playing and obstruction that is going on. Note the Effect for a later task. Spectacular Success will result in the PC being treated like nobility perhaps they are a noble (SOC 11+). Spectacular Failure will result in the PC at the back of every queue, spoken to quite rudely, and dealt with peremptorily.
The second complication is that either forces from a neighbouring polity on a balkanized world, or rebels on a unified government world have decided that this is the moment to make their move in terms of starting a war or making a stand to gain whatever objectives they may have. Theyve chosen PI as a strategic target to take and hold. Perhaps theres a comms tower on the roof to enhance this value (TL35 heliograph or semaphore telegraph tower, TL610 radio mast, TL1114 satellite substation). Any local protection cadre will be overwhelmed or only able to hold out in pockets.
The opponents may be attacking other targets in the city or surrounding territory as well. The Referee can determine when this attack takes place in relation to the PCs progress to mend their finger or can use the table below.
| 1D | PC Situation |
|---|---|
| 1 | A&E Visit |
| 2 | Fracture Clinic |
| 3 | Day Surgery Waiting Room |
| 4 | Day Surgery |
| 5 | Day Surgery Recovery |
| 6 | 2-week followup examination |
If this is not being run as a solo adventure with one Referee and one Player, the other PCs should either be visiting, waiting with, delivering/fetching the PC, or perhaps delivering food or clothing for an extended stay. The stage in the process will determine the PCs incapacity. From 13 the damage is still there but the hand fairly free to function cautiously; 4 the PC will be unconscious; 5 the PC will be coscious but groggy and hand incapacitated (DEX3); 6 the PC will have heavily bandaged hand with some limited use (DEX2). Adjust as appropriate for other tech levels as noted in treatment descri ndash;tions.
Th PCs will hear various rumours to focus their attentions. The Referee may use as many as desirable and should determine if they are true or not.
| 1D | Rumor |
|---|---|
| 1 | All offworlders are being rounded up and shot |
| 2 | All offworlders are being rounded up and taken for interrogation |
| 3 | All offworlders are being rounded up and held captive |
| 4 | The troops are only looking for children |
| 5 | The troops are only looking for those with certain blood types |
| 6 | Demolitions experts have been seen in the basement |
Note the location of the PCs, most obviously in the Orthopaedic & Fracture Clinic or the Day Surgery, but possibly in the restaurant, reception or one of the cafés.
Evacuate!
One of the first three rumours above should be, or if not true, at least apparently true to any direct observation by the PCs and should encourage them to aim to leave the building. They can do this via any of the Entrances but will face an Impossible task throw unless they have some means of either fighting their way out or using some subterfuge. Assume there are 50 troops, four officers and one commander somewhere in the building mainly clustered at key points such as entrances/exits but also at key points such as the Chief Administrators Office or the comms controls. Assume they will be at the PCs present location within five minutes and track the time the PCs take for decisions, any negotiations with staff, and tasks. Rather than track them individually, use the following tasks:
- To traverse a main corridor or move between floors using a lift without encountering opponents:
- Formidable (12+) DEX (1D×10 seconds).
- To move between floors using a stairwell without encountering opponents:
- Difficult (10+) STR (1D×10 seconds).
- To traverse a floor using inner routes without encountering opponents:
- Average (8+) END (1D minutes); BUT add (or subtract) the Effect of the earlier SOC roll to reduce/increase the time if staff are helping or hindering.
Other possibly useful tasks:
- To gain the assistance of staff from one guild, division or cohort:
- Difficult (10+) Leadership/SOC (1D minutes + 5).
- To locate clothes for a disguise (or the injured PC if in gown):
- Easy (6+) INT (2D minutes). Time may be reduced if assisted by staff.
- To create limited amount of explosives with material on hand:
- Easy (6+) INT or EDU (1D×2 minutes).
- To create a large explosion with materials on hand:
- Difficult (10+) Demolitions/INT or EDU (1D×3 minutes). (This can be one task level easier if assisted by staff to find materials.)
- To speak convincingly like a medic for one minute:
- Difficult (10+) SOC (1 minute, INT). (This can be one or even task levels easier if assisted by staff briefing, but the briefing will take twice the length of the performance).
Weapons, if required, may be taken from overpowered soldiers, taken from cadre or a hospital supply, or be the PCs own gear.
The climax of the adventure may be a fight for the exit or a tense deception. If the PCs can make it from the hospital in a vehicle or on foot, assume they can make good their escape to the starport although depending on the exact situation, there may be a heavier security presence at the starport gate. To add to the complications and further the theme of conflict, the PCs may only have escaped to face the larger reality of a looming or erupting interstellar war between neighbouring polities (e.g. the Fifth Frontier War) and need to escape the planet and/or the system.
NPCs
Note there are six options here for a D6 random determination of NPCs. Assume any reasonable medical equipment depending on tech level for the Director, Surgeon and Nurse; assume very little for any patients. Only the Director has been mustered out (although technically not retired yet).
- Hospital Director Marti Forstup
- 785CD9, age 50, rank 6: Director
- Characteristics: STR 7 (+0), DEX 8 (+0), END 5 (-1), INT 12 (+2), EDU 13 (+2), SOC 9 (+1)
- Skills: Admin 3, Diplomat 2, Language 2, Advocate 1, Art 1, Carouse 1, Drive 1, Gun Combat 1, Leadership 1, Mechanic 1, Medic 1, Profession 1, Steward 1, Broker 0, Diplomat 0, Electronics (computers) 0, Science 0, Seafarer 0, Vacc Suit 0
- Cr112,000 Cr45,000 medical bills = Cr67,000, Pension: Cr16,000, Gun, 5 Ship Shares
- Relationships: Ally×5, Contact (criminal)
- Background: Just on the verge of retiring Forstup
has been the director of the Princess Iphigenia for the last 15
years and is highly competent when it comes to the administrative
workings of the hospital and keeping the various factions working
together. Just about. However, now that war has broken out both
internally and externally, the Director is proving uncertain and
indecisive and is accused by some of simply being focused on
retirement plans. The stress is beginning to show and an old and
very serious injury that nearly killed Forstup a couple of decades
previously is suddenly displaying symptoms again.
- Senior Surgeon Filippa Postin
- 9D9589, female, age 38
- Characteristics: STR 9 (+1), DEX 13 (+2), END 9 (+1), INT 5 (-1), EDU 8 (+0), SOC 9 (+1)
- Skills: Medic 3, Electronics 2, Carouse 1, Investigate 1, Profession 1, Science 1, Diplomat 0, Profession 0, Science 0, Seafarer 0, Streetwise 0, Vacc Suit 0
- Background: Postin graduated with honours from
her university and qualified as a physician with a post at Princess
Iphigenia hospital where shes become a senior surgeon of some skill
and reputation. She wears a lucky charm necklace with a strange
design she is convinced helps steady her hand. Shes not wrong, its
an ancient possibly Ancient artifact that gives her a DM+2 to
her already considerable dexterity. Colleagues think shes just
superstitious but she is often called in for the really delicate
cases which others have failed at or regard as impossible. Shes no
nonsense and professional in theatre but out of scrubs knows how to
party.
- Nurse Angar Barcle
- 8576CA, male, age 30
- Characteristics: STR 8 (+0), DEX 5 (-1), END 7 (+0), INT 6 (+0), EDU 12 (+2), SOC 10 (+1)
- Skills: Language 2, Diplomat 1, Medic 1, Science 1, Science 1, Athletics 0, Drive 0, Electronics 0, Investigate 0, Science 0, Vacc Suit 0
- Relationships: Enemies×3
- Background: Barcle seems to rub nigh on everyone
up the wrong way and makes enemies before breakfast. But he knows
his way around the Princess Iphigenia and also has some ability with
language which has come in handy when dealing with patients from
outside the hospitals immediate locality. Hes good looking, knows
it and uses it to his advantage to encourage the sick or injured in
their healing and to chat up fellow colleagues, not to mention one
or two members of the security cadre, in after-hours socialising.
- Caretaker Wilma New
- C79A54, female, age 46
- Characteristics: STR 12 (+2), DEX 7 (+0), END 9 (+1), INT 10 (+1), EDU 5 (-1), SOC 4 (-1)
- Skills: Profession 3, Electronics 2, Jack of All Trades 2, Advocate 1, Engineer 1, Flyer 1, Mechanic 1, Melee 1, Science 1, Admin 0, Drive 0, Medic 0, Profession 0, Science 0
- Background: If you want a tour of the hidden corners of the Princess Iphigenia Hospital, New is the sophont to ask. Shes worked in the place for nearly three decades and can keep anything from cantankerous heating systems to aging medical equipment going. Its a standing joke she spends more time in the Directors office asking for new equipment or additional funds than anyone else in the building, but if she left tomorrow, the place would likely grind to a halt. Its not so well known that in order to keep her and her knowledge, she now earns more than many of the surgeons. Shes tough, shes touchy about damage she thinks is careless, but get on her on side and theres little she wont try and help with.
- Equipment:
At TL5-: None
At TL6+: Mechanical toolkit
At TL11+: Mechanical, Electronics, and Engineering toolkits
- Cadre Commander Gilbon Gettling
- 6B7545, male, age 38, Rank 3: Lance Sergeant
- Characteristics: STR 6 (+0), DEX 11 (+1), END 7 (+0), INT 5 (-1), EDU 4 (-1), SOC 5 (-1)
- Skills: Gun Combat 3, Melee 2, Carouse 1, Gambler 1, Heavy Weapons 1, Leadership 1, Persuade 1, Recon 1, Stealth 1, Athletics 0, Electronics 0, Flyer 0, Tactics 0, Vacc Suit 0
- Equipment:
At TL3: Antique Rifle, Antique Pistol, Cutlass, Flak jacket (troops with Jack armour)
At TL4-5: Shotgun, Revolver, Radio Transceiver (5km), Flak jacket
At TL6-10: Autorifle, Autopistol, Radio Transceiver (5km), Frag Grenades×12, Smoke Grenades×6, Mesh armour
At TL11+: Advanced Combat Rifle or Laser Carbine, Auto Pistol or Laser Pistol, Radio Transceiver (Computer 0, 500km), Commdot, TL10 Stunner, Stun Grenades×12, Cloth armour - Background: After dropping out of military academy, Gettling still managed to join the marines but was injured and forced to muster out. He enlisted in the planetary army as infantry and carved out a small career for himself eventually being put in charge of the small cadre of soldiers protecting the Princess Iphigenia hospital. Not a high value target or a high value posting. He is short and stocky with a pockmarked face but a can do attitude that sometimes takes a risk too far.
Patients
Roll D66 on the Above the Crowd table and inflict D3 rolls on the Injury table (Core Rulebook Update 2022 p.49) to establish the patients current status. This may determine whether theyre in theatre, intensive care, or recovery wards; or use the Treatment Stage table given in the adventure.
Equipment
Bone Saw:
A surgical saw for amputations. As a weapon, 1D+3 damage but with a bane in attacks for its awkwardness.
Crutches:
Wooden, or at later tech levels aluminium or other advanced materials (e.g., carbon fibre), crutches to assist patients in recovery from leg injuries or replacement with prosthetics. They may be used for extended periods of time by those who find prosthetics limited or difficult to adjust to. Grav chairs may become an option at TL11 or higher. Note Prosthetic options in Central Supply Catalogue, p.87.
Artificial Leech:
A metal cylinder for use when live leeches are unavailable or undesirable. Rotating blades cut the skin as the tube suctions blood from the patient.
Tablet Dispenser:
A plastic (or at lower tech levels wooden but much larger) box for tracking and dispensing any drugs a patient might be taking. Particularly useful if multiple regimes or strict timings are required.
Minor Surgery Toolkit:
Scalpels, blades, forceps, skin hooks and retractor for examination, minor surgery and suturing.
Gene Editor:
Enables the sequencing of an individuals genome and the cutting of a genome at a desired location too allow genes to be removed or new ones added. This offers cures for diseases, cancers and genetic abnormalities. It can be used to create new medicines, agricultural products and genetically modified organisms. Some high Law Level worlds ban their use. At TL11 six treatments can be performed with one charge. Nuclease refills enable a further six treatments. At TL11 treatment takes 1D hours; at TL14, 1D minutes. N.B.: Not available at TL10-. Typically, Traveller tech level tables dont allow genetic engineering until TL14 (e.g., LBB9: Library Data), in which case, use the TL11 numbers below as the TL14 introductory costs and the TL14 figures as TL15 technology. Referees may also wish to consider the ramifications of making this kind of technology freely available, but see also John Sneads thoughts on the subject in the section on Biotechnology in his article Traveller for the 21st Century.
| Item | TL | Mass (kg) | Cost |
|---|---|---|---|
| Bone Saw | 2 | 1 | Cr100 |
| Crutches | 2 | 2 | Cr50 |
| Artificial Leech | 3 | 1 | Cr150 |
| Tablet Dispenser | 6 | - | Cr5 |
| Minor Surgery Toolkit | 6 | 1 | Cr500 |
| Gene Editor | 11 14 |
10 2 |
Cr10,000 Cr1,000 |
| Nuclease Refills for Gene Editor | 11 14 |
- - |
Cr1,000 Cr100 |
Factions for Medivac!
The adventure makes reference to medical staff being divided into Guilds, Divisions or Cohorts depending on tech level, but little further detail is given save to say that theyre identifiable by various methods. (See the fifth paragraph under Referees Information).
The idea of these factions is to give further opportunities for role playing as the different groups interact with each other and perhaps make things harder for the PC(s) who are caught up between them at various points. As the text notes, relationships have broken down which should provide additional conflict. This reinforced the theme of war for the competition the adventure was submitted to. It should be noted that although the scenario is inspired by a real-life accident and its subsequent treatment, the staff I met were nothing but professional, kind and helpful.
The various names given to the groups are completely arbitrary but perhaps redolent of the tech levels theyre suggested for. They can be swapped or replaced as desired. The adventure envisions them being divided by medical discipline but other arrangements are possible: traditionalists vs technology adopters; researchers occupied with the theoretical vs patient carers more concerned with the practical and the here and now; ethicists vs progressives in institutions where complex issues are being dealt with and some prioritise scientific progress over ethical concerns or vice versa; it could even be that different physical locations in the building have become the scenes of strife perhaps the different floors for example.
Examples (may need to adjust for tech level)
The staff in the emergency department see E3 on the map (A&E accident & emergency, or ED emergency department, or ER emergency room or Casualty) are seen as risk takers and adrenaline junkies who make dangerous choices for patients. Of course, they see the staff working in internal medicine as staid and too cautious in critical situations. There are similar arguments between the oncologists advocating, so its said, overly aggressive treatment options and those involved in palliative care emphasising quality of life and pain management for terminal illnesses. This is so emotionally charged due to nature of the patients that many other staff have been involved in protests and blockades which may be encountered by PCs on any given day on a 1D roll of 5+.
The obstetricians at PI are at loggerheads with neonatology as the former focus on maternal health during pregnancy and delivery and feel resources should be focused in these areas to get the best outcomes, and the latter deal with premature births and expect large allocations of resources to support newborns with complex medical needs. Both groups have been massaging submissions to finance to slant requisitions their way, but theres also been some tit-for-tat pilfering of equipment and minor acts of sabotage sometimes from other departments around the hospital to replace whats been taken or broken.
Recently, there were actual fisticuffs between the psychiatrists and the neurologists who might both work with the brain but approach mental health from different angles. The psychiatrists were accusing their opponents of overemphasising physical treatments and carrying out unnecessary procedures, while the neurologists retorted that too much medication was being prescribed and achieving very poor outcomes. A lunchtime seminar on The Mind: Inputs or Outputs? by a renowned visiting professor Dr Ardua Starling largely ignorant of the situation, moved from debate to debacle and several delegates ending up in A&E.